
Anterior Cruciate Ligament (ACL) Injuries
An ACL injury affects the anterior cruciate ligament in the knee. This ligament connects the thigh bone to the shin bone and helps keep the knee steady when you move. It is especially important for twisting, turning, and quick changes in direction. When the ACL is injured, the knee may feel painful, swollen, and unstable during everyday activities and sports.
On this page, you will find out how common ACL injuries happen, the different types and levels of tears, and how they are diagnosed. We also cover treatment options, recovery timelines, and what to expect during each phase of ACL rehab. The goal is to help you understand your injury, know what comes next, and feel confident moving forward.
OVERVIEW
The anterior cruciate ligament (ACL) is a strong band of fibrous tissue located deep in the center of the knee. It connects the thigh bone, called the femur, to the shin bone, known as the tibia. The ACL plays a key role in stabilizing the knee during movement.
ANATOMY
An ACL tear can happen with or without contact from another person. It usually occurs when the knee twists suddenly or bends too far backward. These strong forces put too much stress on the ligament and cause it to tear. These strong forces put too much stress on the ligament and cause it to tear. When sustaining an acute ACL tear, 68% of athletes were injured by a non-contact mode of injury, 32% were injured by a contact mode of injury. Overall, female athletes are 2 to 8 times more likely to experience an ACL tear than their male counterparts. This range is dependent on age, hormone levels, sport, level of intensity of sports competition, and individual risk factors. Understanding how these variables interact helps explain why ACL injuries are so common in athletics and why prevention strategies often focus on movement patterns, strength training, and neuromuscular control, especially for female athletes.¹
MECHANISM OF INJURY
-
A Grade I sprain is a mild injury where the ligament is stretched a little and has tiny tears. It may feel sore, but there is very little pain and the joint still feels mostly stable. This type of sprain is usually treated with rest and simple conservative care, not surgery.
-
A Grade II sprain is a moderate injury where the ACL ligament is partly torn. It usually causes noticeable pain, swelling, and the knee joint may feel unstable or wobbly. Treatment can include physical therapy and rest, and in some cases surgery may be needed.
-
A Grade III sprain is a severe injury where the ligament is completely torn. It causes a lot of pain and swelling, and the knee joint may feel very unstable or unable to bend. This type of injury is usually treated with surgery to repair or replace the ligament.
-
A Tibial Spine Avulsion Fracture happens when the ACL pulls a small piece of bone off the top of the shin bone. This injury is more common in kids and teens whose bones are still growing. It can be treated with a brace if the bone stays in place, or with surgery if the bone has moved.
TYPES OF INJURY
-
Diagnosing an ACL tear with an MRI or X-ray means taking images of the inside of the knee. An MRI shows the ligaments and can clearly tell if the ACL is torn, while an X-ray shows the bones and checks for fractures. These images help doctors confirm the injury and choose the best treatment.
-
A special test or clinical exam is when a healthcare provider uses their hands to examine the injured knee joint. They gently move your leg in certain ways to see how it moves, where it hurts, and if it feels stable. This helps them understand what part of the knee is injured and how serious the injury is.
-
The healthcare provider will ask the patient about their symptoms. This includes how the injury feels and how it affects daily activities, such as pain, swelling, weakness, or trouble walking, running, or playing sports. These answers help the provider understand how the injury is affecting the patient’s normal life and recommend the best treatment to support recovery.
DIAGNOSIS
TREATMENT TIMELINES
Conservative Treatment (3-12 months): means helping the knee heal without surgery, usually over 3 to 12 months. It can include rest and protection, using crutches to reduce weight on the knee, wearing a brace, taking medicine for pain and swelling, and doing physical therapy. As healing improves, treatment also includes strength training and exercises to help the person safely return to sports.
Surgical Reconstruction (9 to 18 months): means having surgery to rebuild a torn ACL, and recovery usually takes about 9 to 18 months. The new ligament can be made using tissue from your own body, called an autograft, such as the hamstring, quad, or patellar tendon, or from a donor, called an allograft. Your doctor will choose the best option based on your age, activity level, body type, and what will help you heal and return to sports safely.
GRAFT TYPES
Allograft: An allograft is a tissue graft from a donor of the same species (cadaver) as the recipient, but not genetically identical. Allograft options are typically tendon grafts from hamstring, tibialis posterior/anterior, or Achilles tendon.
Autograft: An autograft is a graft of tissue from one point to another of the same individual's body. There are three main sources of autograft: bone-tendon-bone (BTB) graft of the patellar tendon or a tendon graft from hamstring or quadricep tendon.
EARLY ACL REHAB
What to expect in your first few weeks following knee surgery
After knee surgery, the first few weeks are all about staying safe and helping your knee heal. During this time, you will focus on moving carefully, resting enough, and controlling your swelling and pain. You will also learn what warning signs to watch for so you can get help quickly if something does not feel right. These early steps help protect your knee and set you up for a successful recovery.
-
Prevent Falls by making clear walking paths in your home, especially if you will be using a walker, crutches, or a cane after surgery. Move furniture out of the way and remove tripping hazards like extension cords and area rugs to help you walk safely.
-
Limit your trips out of the house to prevent overdoing it leading to increased pain, swelling, and stiffness.
-
Keep an eye on your injured knee size as you heal. The goal is to get the swelling down to within about 1 to 2 centimeters of the circumference of your other knee. Elevate your leg up above heart level, and wear a compression wrap or sleeve. Ice for 10 to 20 minutes at a time, 3 to 5 times a day (or more). These four things can help bring the swelling down.
-
Take your pain medicine exactly as your doctor tells you. When you no longer need prescription pain medicine, you can use over-the-counter pain relievers if your doctor says it’s okay. Changing positions every 45 minutes, keeping your leg elevated and using ice can also help reduce pain.
-
Keep your incision clean, dry, and covered, and watch for signs of infection. Call your doctor right away if you notice more drainage, redness, pain, warmth, or a bad smell around the incision. Check your temperature every day and contact your doctor if it goes above 101°F.
-
Watch for signs of blood clots. Help prevent them by walking, doing your home exercises, elevating your leg, and using compression stockings or blood thinners if your doctor prescribed them. Call your doctor if you notice a big increase in swelling in your thigh, calf, or ankle that does not go down with elevation, or if your calf feels tender or painful.
ACL REHAB PHASE - I
You should have received an ACL Rehabilitation Protocol from your surgeon, if not please ask your physical therapist as they may have a copy to share with you.GOALS: Week 1
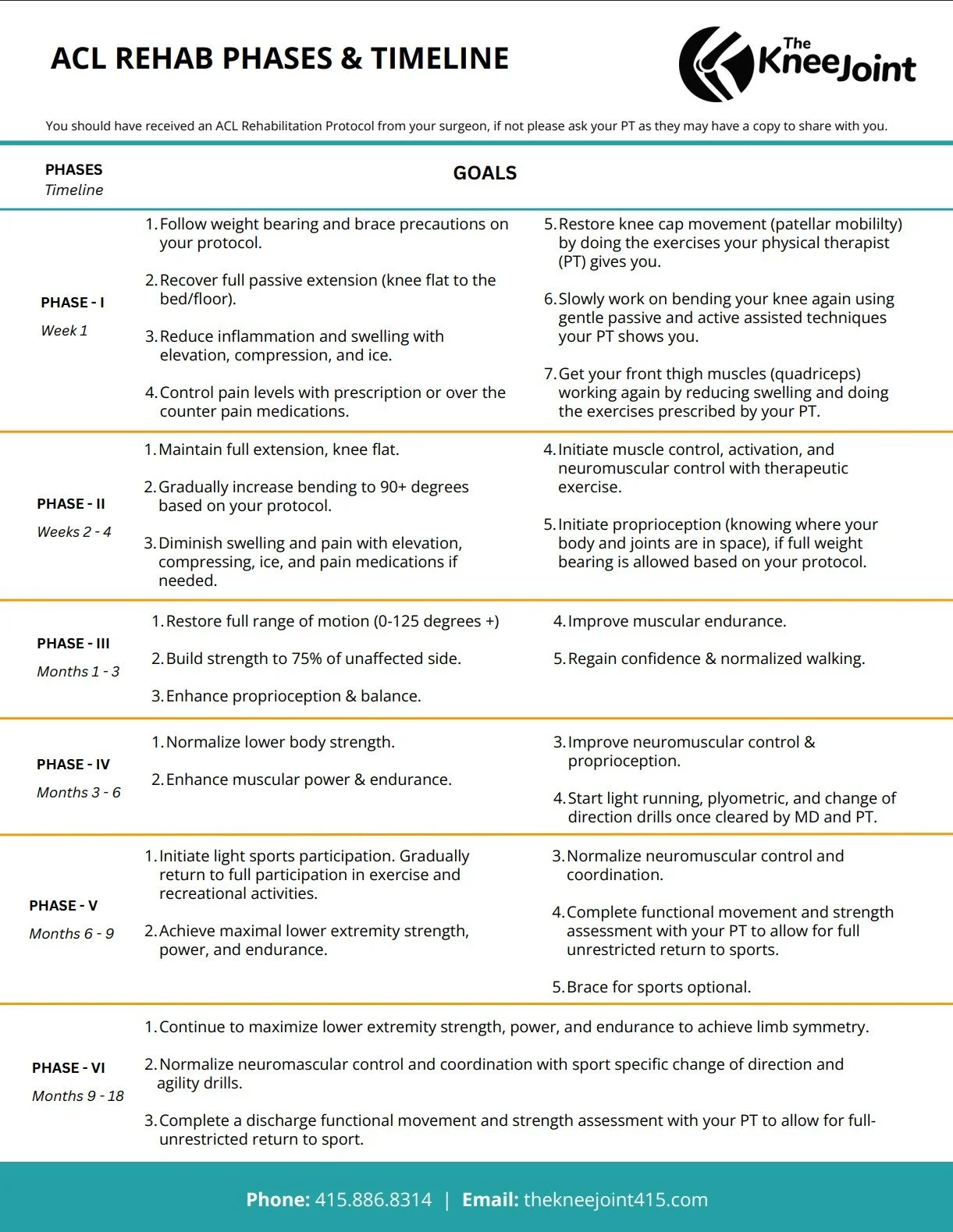
Follow weight bearing and brace precautions on your protocol.
Recover full passive extension (knee flat to the bed/floor).
Reduce inflammation and swelling with elevation, compression, and ice.
Control pain levels with prescription or over the counter pain medications.
Restore knee cap movement (patellar mobility) by doing the exercises your physical therapist (PT) gives you.
Slowly work on bending your knee again using gentle passive and active assisted techniques your PT shows you.
Get your front thigh muscles (quadriceps) working again by reducing swelling and doing the exercises prescribed by your PT.
ACL REHAB PHASE - II
You should have received an ACL Rehabilitation Protocol from your surgeon, if not please ask your physical therapist as they may have a copy to share with you.GOALS: Week 2 - 4
1. Maintain full extension, knee flat.
2. Gradually increase bending to 90+ degrees based on your protocol.
3. Diminish swelling and pain with elevation, compressing, ice, and pain medications if needed.
4. Initiate muscle control, activation, and neuromuscular control with therapeutic exercise.
5. Initiate proprioception (knowing where your body and joints are in space) , if full weight bearing is allowed based on your protocol.
ACL REHAB PHASE - III
You should have received an ACL Rehabilitation Protocol from your surgeon, if not please ask your physical therapist as they may have a copy to share with you.GOALS: Month 1 - 3
Restore full range of motion (0-125 degrees +).
Build strength to 75% of unaffected side.
Enhance proprioception and balance.
Improve muscular endurance.
Regain confidence and normalized walking.
ACL REHAB PHASE - IV
You should have received an ACL Rehabilitation Protocol from your surgeon, if not please ask your physical therapist as they may have a copy to share with you.GOALS: Month 3 - 6
1. Normalize lower body strength.
2. Enhance muscular power & endurance.
3. Improve neuromuscular control and proprioception.
4. Start light running, plyometric, and change of direction drills once cleared by MD and PT.
ACL REHAB PHASE - V
You should have received an ACL Rehabilitation Protocol from your surgeon, if not please ask your physical therapist as they may have a copy to share with you.GOALS: Month 6 - 9
1. Initiate light sports participation. Gradually return to full participation in exercise and recreational activities.
2. Achieve maximal lower extremity strength, power, and endurance.
3. Normalize neuromuscular control and coordination.
4. Complete a functional assessment with your PT to allow for full-unrestricted return to sports.
5. Brace for sports optional.
ACL REHAB PHASE - VI
You should have received an ACL Rehabilitation Protocol from your surgeon, if not please ask your physical therapist as they may have a copy to share with you.GOALS: Month 9 - 18
1. Continue to maximize lower extremity strength, power, and endurance to achieve limb symmetry.
2. Normalize neuromuscular control and coordination with sport specific change of direction and agility drills.
4. Complete a discharge functional movement and strength assessment with your PT to allow for full unrestricted return to sport.
ADDITIONAL RESOURCES
The Knee Joint EARLY ACL REHAB Guidelines
This printable PDF one sheet includes information about what to expect in your first few weeks following knee surgery. Download and reference it whenever you’d like support, want to build momentum and feel focused in your recovery journey.
One Sheet
The Knee Joint ACL REHAB PHASES & TIMELINE
This printable PDF one sheet includes information about what to expect in the weeks and months following ACL surgery and rehab in addition to goals to keep in mind as you progress from Week 1 to Month 18. Download and reference it whenever you’d like support, want to build momentum and feel focused in your recovery journey.
One Sheet
Blog Post
Instagram References
Why Are Women More Likely to Get ACL Injuries? Instagram · @natgeoscience
Protect Your ACL Instagram · @teamacl_ and @fckruisband
Teenage Girls Are Most Likely To Tear Their ACLs. Parents Say More Must Be Done To Protect Them. San Francisco Chronicle · Marc Levy, Associated Press
Article
¹ Tjong V. Why Women Have More ACL Injuries Than Men. Northwestern Medicine HealthBeat. https://www.nm.org/healthbeat/healthy-tips/why-women-have-more-acl-injuries-than-men. Accessed March 9, 2026.